
 Only days to go in the countdown to the publication of the worlds most expensive doorstop DSM5.
Only days to go in the countdown to the publication of the worlds most expensive doorstop DSM5.
If you really do need a doorstop try your local dollar store – mine has two for $1.29 and they work perfectly well.
On the other hand, if you’re waiting eagerly to find out just how crazy you are, or how many mental disorders you qualify for, or simply need something solid to sit on, then hang on just a few more days – it’s out next Wednesday.
DSM Diagnostical Statistical Manual of Mental Disorders is published by APA American Psychiatrc Association next week.
If you start lining up now, you’ll be alone – very alone – for over a week but you may just qualify for bonus disorders.
Its my party and I’ll cry if I want to
Witness, if you will, the jostling for position to claim a seat at the table for who gets to write the next one. Competition is rife and very public over who gets to define how we are supposed to understand how human beings go mad; what words we use; who gets to dish the dirt, dole out research grants and decide who gets to research what with money that could otherwise go to services that might actually help people who need it.
DSM also plays a big part in the lives of the many academics who make a living studying, teaching and publishing on the basis of their opining on the effects of all those categories of madness listed in DSM, the impact on us, society and, well, whatever they can get a grant for rabbiting on about.
And it’s not just docs, and academics but social workers: community workers, in fact a whole host of worker workers, even teachers, who get trained to “spot” those tell tale “signs” and to think only by categorising human behaviours in terms of the dozens of disorders indexed in DSM.
Then there’s a whole host of somebody’s taking it upon themselves to ask us if we’ve taken our meds, they obviously need to know how to spot the signs we haven’t done so.
 Beyond all that DSM feeds deep basic assumptions rife in our society that those of us who don’t quite fit, or struggle to live in a chaotic world must have a ment disorder that requires to be managed by drugs so others can feel safe living on the same planet as us.
Beyond all that DSM feeds deep basic assumptions rife in our society that those of us who don’t quite fit, or struggle to live in a chaotic world must have a ment disorder that requires to be managed by drugs so others can feel safe living on the same planet as us.
All this is to say nothing of the professions jostling like only professional jostlers can, to sit in the clinician’s big comfy chair so they can get paid for helping us heal our wounded souls when we need their expert help healing our wounded souls.
And lets face it, APA has made it seem so easy and so, so random to diagnose each other that we can all have a go. Diagnosis bt numbers.
Many of us even like to have a go at making up new ones ourselves. Like this guy said.. Oo Madam! Titter ye not.
.
The Big book of Fairy Tales

.
Mad? you betcha
Most of the world uses a different index – the ICD or International Classification of Diseases published by WHO -World Health Organisation but in North America we know better because we’re bigger and so we use our own – or in Canada we borrow America’s own. There is no CanCon in mental health we just copy America – we just do it in the basement and a bit slower. China has its own system too. DSM – Diagnostical and Statistical Manual of mental Disorders is the reference index for the classification of “mental disorders” in Canada so that longest undefended border is also undefended against the world’s daftest system of going mad..
Seriously, with all the initials in mental health you’d think there was a serious epidemic of disorder about.
 The DSM is also, more often than not, prefered by researchers worldwide to plonk people – or “subjects” as they so kindly call us – into categories so they can study us like lab rats. Yes rats, the parrots are dead. Clinical psychologists like pigeons. Me, I prefer the Dove From Above [see above].
The DSM is also, more often than not, prefered by researchers worldwide to plonk people – or “subjects” as they so kindly call us – into categories so they can study us like lab rats. Yes rats, the parrots are dead. Clinical psychologists like pigeons. Me, I prefer the Dove From Above [see above].
So, this way the assumptions built into DSM inform all psychiatric research and practise, all mental health services [because they are essentially adjuncts to psychiatry] and, more and more, our everyday understanding of being human – and all round the world, not just in North America. Try Reading Ethan Watters – he wrote a great book – “Crazy Like Us”-about how America ia colonising the way the world goes mad. The DSM is a key tool in that.
What’s a mental disorder?
Well, no one really knows – at least no one who is honest about it – but the APA has the Texas ranch-sized hubris to think they do. At any rate, the APA pretends to know a lot more than anyone else even though they have a hard time producing any scientific evidence of knowing anything at all except how to get drug companies to give them loads-a-money. There’s lots of evidence that getting drug companies to give them loads-a-money is something at which they are very good indeed. I expect they could make some extra coin from running seminars on how to do it.
So, if we don’t know what a “mental disorder is how come someone keeps creating new ones and classifying them in such a big, indigo book?
Good question but it involves a lot of committees, a lot of schmoozing paid for by pharmaceutical industry and a lot of golf. Essentially, members of APA sit round on committees, propose stuff and vote on it til they get so bored they turn crazy – enough they almost diagnose each other. Somewhere along the way the private club known as the APA decided they were in charge of that process.
The really crazy thing is that the rest of the world let them.
.
Diagnosis uh! what is it good for?
-absolutely nothing! say it again! Well the point of a diagnosis is that its a kind of shorthand for a recognisable condition that a bunch of humans might get. It might help us understand – might even bring us the comfort of knowing “phew! it’s not just me!”
Well the point of a diagnosis is that its a kind of shorthand for a recognisable condition that a bunch of humans might get. It might help us understand – might even bring us the comfort of knowing “phew! it’s not just me!”
Perhaps most importantly, a diagnosis is supposed to indicate those treatments that are known to work reliably to alleviate the condition described.
In the end a diagnosis is just a hypothesis – a testable idea that your doc thinks your problem is disorder x, therefore best treated with treatment options y, z etc., which if you are lucky may be available to you without having to wait til the Leafs with the cup again.
the problem is the categories were just made up, mostly by a bunch of blokes sitting round in smoke filled rooms – the categories bear less and less resemblance to the real world every day, yet APA and many others cling to the categories as though they are more real than real – surely that’s highly diagnosable?
Anyway back to you and your Doc – How do you know if your Doc’s hypothesis is true?
Well, if the drug works then the Doc was right.
If it doesn’t work and your Doc – and you – are patient enough then you try again and keep trying till you find one that works better than the others you tried.
If your Doc is not patient or insists he is right, or if you resist then you will likely get blamed and told that you’re not taking the meds properly or that you need to take more , and more different drugs until they do. You may get told that you “lack insight”, are “non-compliant”, untrustworthy, lying, an alien, a spy or just a plain ol pain in the ass. You may then “qualify”for depot injections – large weekly or monthly doses in the ass – or arse depending on which side of the Atlantic yours happens to be.
If your meds continue to fail to prove that your Doc is right then you may be termed “treatment resistant” – which basically means that you have caused the complete and total failure of the entire health system – yes, it’s your fault.
If you’re lucky, then you may get banished from the hospital but it usually means that you get the really special drugs that they don’t just give to anyone with any old disorder because they are really scary. That or you get electroshock. Whichever option we know even less about these than the othe lot, especially the harm they can do. And, of course, by now they’ve found a way to remove your right to choose.
Remember, in this system, the Doc cannot possibly be wrong and the drugs cannot possibly not work – so if they don’t work for you then it’s simply your fault.
It simply is not possible that the Doc can be wrong or that the drugs are crap.
Resistance is futile, and always leads to more diagnoses and more drugs. Yay for drugs!
Who needs a diagnosis?
Well, actually no one. But it might help to get access to services. Your Doc will write a code on your paperwork – the ICD code – for whatever diagnosis he or she might hypothesise best fits your complaint.
What, the ICD code? Yes they diagnose you with DSM but the equivalent ICD code is the one that goes one the paperwork. That’s so that the WHO can monitor your progress- well not yours but whole populations of folks diagnosed and taking drugs. See, the ICD and the DSM are not really that different. The ICD is actually a huge Matrix-like computer programme that controls the entire world: go ahead, Google it.
It’s worth noting that if you need a note from your Doc to excuse you from work or other duties then your Doc does not have to write your diagnosis on that note – they can simply write “medical reasons”. Go Doc.
 Mostly your doctor needs a diagnosis so that they can put it on the paperwork and get a chit to get paid for diagnosing you. They can also get a chit to get paid for sitting in the big comfy clinicians chair listening to your crap, and for writing prescriptions for drugs and stuff so can hopefully you feel less bad about your crap, though you may also still feel like a zombie or like Johnny on a bad day.
Mostly your doctor needs a diagnosis so that they can put it on the paperwork and get a chit to get paid for diagnosing you. They can also get a chit to get paid for sitting in the big comfy clinicians chair listening to your crap, and for writing prescriptions for drugs and stuff so can hopefully you feel less bad about your crap, though you may also still feel like a zombie or like Johnny on a bad day.
Your medical insurance company, if you have “coverage”, needs a diagnosis so they know how to screw you and pay out the smallest possible amount for the shortest possible time.
The government needs a diagnosis so that they can do whatever they do. Just don’t ask them what they do: they’ll spend a fortune of consultants trying to work it out, then hide the report for years till they can find someone to pin the blame on – that person will then likely need expert help to heal their wounded soul too.
.
What tests will the Doc do to diagnose a mental disorder?
There are no mental disorders that have any medical diagnostic tests.
None.
They will not need your blood, or any other fluids, nor will they need to cut bits off you or out of you. In fact, so confident in the biology are they that they don’t actually need to use biology to diagnose mental disorders – they use checklists instead.
You can find the same checklists on the internet – or just make them up they’ll be just as scientific. Sometimes they have extra special secret checklists that you can’t get your hands on – checklists with more, special secret agent questions that you need to be specially trained to operate without being a danger to society. It’s a bit like how only plumbers can get the special tool to take out the valve so you have to call them out and pay them hundreds of dollars to use their “experts only” tool.
 So what about all those fancy pictures of brains, don’t I get a picture of my brain?
So what about all those fancy pictures of brains, don’t I get a picture of my brain?
Nope.
If you like this one, consider it yours.
.
No blood?
Not unless you think you’re a vampire, which is not in the book – though worrying exessively for more than two weeks that you have physical symptoms of becoming one, is. While we’re on it, worrying about being a vampire is pointless – if you are one you’ll know.
Actually, it may well be worth requesting your Doc to run blood tests for vitamin and mineral deficiencies – vitamin deficiencies can, in Doc speak “mimic” “mental disorders”.
There also are many illness that have similar symptom profiles to many mental “disorders” and many of these do have real tests and reliable courses of treatment.
Many psychiatric medications can result in patterns of side effects that exactly repeat the symptom lists of mental disorders other than the one its meant to be treting you for. This is the Catch 22 that can lead to you being trapped in multiple diagnosis and poly-psychopharmatherapy.
Polypsychopharmatherapy is a big word for being told to take a shit-load of drugs for the rest of your life – and is what most psychiatrists, especially in “the healthcare system”, actually practice. Medicine and psychiatry -a specialism within medicine – are supposed to be much broader than just writing chits for drugs and in practice as much an art as a science. Even many of those in psychiatry who would prefer to practise in other ways feel they are constrained and compelled -sometimes by law] to limit themselves to the practise of polypsychopharmatherapy.
If there are hundreds of disorders, why does everyone gets the same four drugs?
Again, good question.
Well, yes, there are hundreds of “mental disorders” listed in DSM and yes there are only four basic types of psychiatric drugs – even the “new” ones are just variations on the old ones.
Mostly, new psychiatric meds are variations on the same old drugs just sold with a fancier name and a claim to have “fewer known side effects”. Newer ones are typically called “atypical” probably because “new” sounds like we don’t yet know what the side effects might be – which would give the game away.
Note that the main reason new drugs have fewer known side effects is that we find out about most side effects only after new drugs have passed trials and been put onto the market. Besides the kind of side effects that kill instantly, the most reliable [only] way we find out about most side effects of drugs is after thousands of people like you and me have trusted their Doctor and been using them for a while – and, oopsy! we find there are nasty side effects.
51% of all prescription medicines have known harmful side effects
Every drug is experimental- even if it works for everyone else alive I don’t know how it will work for me until I try it. Same goes for you.
 If you’re lucky you might find a version of one of the four drugs that helps you feel better without making you also feel like shit, or feel nothing at all, like a zombie; causing you to put on 100lbs in three minutes; and does not leave you wanting to pull the fingernails off everyone you meet or so anxious you’ll explode if you don’t, right now, do to someone what Laurence Olivier did to Dustin Hoffman in Marathon Man.
If you’re lucky you might find a version of one of the four drugs that helps you feel better without making you also feel like shit, or feel nothing at all, like a zombie; causing you to put on 100lbs in three minutes; and does not leave you wanting to pull the fingernails off everyone you meet or so anxious you’ll explode if you don’t, right now, do to someone what Laurence Olivier did to Dustin Hoffman in Marathon Man.
Most trials for psychiatric drugs have difficulty proving that the drug is more effective than placebo – which is basically means that the medication is not much more effective than a sugar pill that your Doc has told you will help you feel better.
So why don’t they prescribe placebo?
Well in some countries, like Germany, Docs do prescribe placebo – they also prescribe herbs and exercise for depression, which you may not like. American doctors think herbs is cheating and real medicines only come from labs and factories. Generally, in N. America its actually illegal to prescibe placebo – something or other to do with Doctors cheating and snake oil salesmen. Anyway placebo is and sugar sugar is bad for you too and big sugar is well dodgy just like bit tobacco, big oil, big pharma.
But don’t I have a “chemical imbalance”?
And if your Doc says you have a “chemical imbalance” then you tell them straight up that you know that they know that’s a crock of shit, and you know who told them to tell it to you: that nice drug company rep who visits them with samples and a nice lunch.
If you are one of the lucky one-in-seven who find that the drugs do help you then it’s not because they correct anything. They might well change the way you feel about the crap in your life, and you may decide that living with the side effects you experience is worth that: you get to choose.
 But the drug is not “correcting” a “chemical imbalance”.
But the drug is not “correcting” a “chemical imbalance”.
If you get a headache and you take a Tylenol and the headache goes away, you don’t conclude that the headache was caused by Tylenol imbalance.
You know that would not be a real scientific deduction.
It’s the same with psychiatric meds. The “chemical imbalance” line was invented for your Doc to tell you so that you would keep taking the meds and get out of their surgery quickly.
How come the only help I get offered is drugs, more drugs and even more drugs?
 Well, basically public funded medicine has for the last few decades been dominated by people interested in drugs. No mystery, really but it does mean that other methods have been forced to take a back seat, people involved find it hard to get funding for services or even to research non-drug methods that might help so that we can build evidence of how they do. So we’re left with more drugs.
Well, basically public funded medicine has for the last few decades been dominated by people interested in drugs. No mystery, really but it does mean that other methods have been forced to take a back seat, people involved find it hard to get funding for services or even to research non-drug methods that might help so that we can build evidence of how they do. So we’re left with more drugs.
There’s also the fact that your Doc can write a prescription for drugs in a few minutes, whereas most of the other stuff takes a lot of time. In Ontario, most Docs get a fixed fee payment for the appointment and then another fixed fee payment per prescription – so they are actually incentivized to prescribe drugs. Yes, at an average $340k gross per year in Ontario your Doc is a piece worker just like the young lady who sews your pants together in Bangladesh.
Also, don’t forget many of us go to the Doc expecting and asking for drugs. As a society we like drugs. We’ve come to expect that taking a pill is about the hardest we need to work to fix whatever crap we might have in our lives: take-pill-make-crap-go-away is our prevailing philosophy.
Seriously, we know full-well that the Doc has special powers to fix us and special access to special to drugs that we can’t get on the high street – neither from a regulated nor unregulated retailer.
So what else can I do?
Well, there likely are many other things we can do that will help but it’s such hard work: if you went to the Doc and they told you that you could take a pill ; or you could spend the next two-to-twenty years, in serious reflection and hard work, re-learning how to live, sorting out all the things in your life that leave you feeling so crap, what would you do?
There’s a good chance, you’ll try the pills first – they might even help you get started with that self-reflection and hard work stuff till you get the hang of it.
What if I have money to pay?

They are out there, there are many of them and they are happy to work with you. Most of them will ignore DSM and the more you pay them the more they will ignore DSM. Note you will likely need a more moolah than shown here.
.
.
Anyhoo, the APA publishes its latest edition DSM5 next week and its raising some right old hoo-har.
.
Who or what is the NIMH and why are they saying the DSM has no validity?
Ok, NIMH – National Institute of Mental Health is a bureaucracy in US that amongst other things dishes out money for research that is supposed to help with mental health. They are very close with the major drug industry and academics who research drugs and others who like big expensive toys. NIMH also fund bodies that will psychoeducate you about what’s wrong with you and how you can be fixed by experts who can get you a note for drugs and another note for time off work.
Last week, even these guys came out and said DSM is pretty well useless for organising even biological research into mental health problems – that it has little scientific basis and is, well, really not very useful.
NIMH says the science behind DSM is, really, well not very good: not based in real biology, and leads to drugs that are, well, really not very good either. NIMH analysis is that current biology and drugs are not very good – they think what we need is more research into biology and more drugs.
They believe we are merely ten years away from a big breakthrough in understanding how biology makes us mad.
We’ve been only ten years away from a big breakthrough in understanding how biology makes us mad for the last sixty years. Mad, eh?
The profession of psychiatry has a long [and largely pretty dark] history of pretending to be the world’s leading expert in madness – biology and genetics is simply their latest favourite theory. Remember its not that long ago they said homosexuality – it’s bit longer but notreall that mush but they also used to dsay that black slaves trying to escape white masters diagnosably mad.
Really, NIMH mostly want to be in charge of the sandbox and to have all the money and be be left to get on with doing science like playing with flies and taking pics with fMRIs for another twenty or thirty years til they can retire.
Meanwhile, we can take those four drugs that they tell us are, well, really not very good.
“PAtients Deserve better” is what the guy said.
.
Who is the BPS and why do they say the DSM is pretty much redundant?
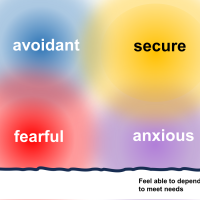
BPS is the British Psychological Society. Today they said that there is no scientific basis underpinning the idea that serious mental illnesses like “bipolar” and “schozophrenia” have a biological basis – or even that they exist at all. They call for a total paradigm shift in how we view mental health and “mental illness”. “Paradigm shift” is a fancy way of saying “big change”.
They say that DSM and the whole basis upon which it is built is not very useful for understanding what people might experience and even less useful for helping them when they do.
 In a nutshell, psychologists believe – and some have been doing research to demonstrate it – that mental health difficulties are caused more by the shit that happens to us than they are programmed or determined by our genes.
In a nutshell, psychologists believe – and some have been doing research to demonstrate it – that mental health difficulties are caused more by the shit that happens to us than they are programmed or determined by our genes.
They believe it’s mostly the world we live in that makes us mad.
Psychologists like talk therapy, of which there is an infinite variety of types but they all basically work by you talking about your shit while they get paid to listen and promise not to tell anyone. They might not promise not to laugh, though the good ones will have a few good jokes too. The really good ones are likely even more mad than you but are doing a pretty good job at getting on with life – and not afraid for the world to know it.
.
Who or what is Mad Pride International and why are they asking me to think of funny things to do with a DSM?
 Mad Pride is a bunch of folks who think this is all bloody bonkers, that maybe even it’s destructive and what is making us mad in the first place.
Mad Pride is a bunch of folks who think this is all bloody bonkers, that maybe even it’s destructive and what is making us mad in the first place.
If DSM5 is being declared to be without basis and pretty much useless even before its published, what would you do with it?
Seriously, it’s a bit of silly fun – how many uses can you come up with for a DSM5?
https://www.facebook.com/groups/MadPrideInternational/
.
How Come The Guardian is so interested and the Globe and Mail isn’t?
Yes the Guardian published three articles yesterday alone – and there were two pieces on BBC radio today.
Meanwhile, in Canada it’s May so we’re watching summer sports – hockey – and planning for summer…and beside who knew the leafs would be so unsucky? Go Leafs!
postcript: oops! the Leafs suck again.
- Does mental illness exist? http://www.guardian.co.uk/society/2013/may/12/medicine-dsm5-row-does-mental-illness-exist
- Do we need to change the way we think about mental disorders? http://www.guardian.co.uk/science/2013/may/12/dsm-5-conspiracy-laughable
- another one.






























































































Hi there, Recovery Network: Toronto. Great overview of the DSM topic. You might be interested to know that here is a group of internationally influential people who agree that the DSM is indeed deeply flawed and are seeking to come up with a humanistic alternative to the DSM. Those of you who might want to make some comments on specific alternative can go to the site at DxSummit.org. I’ve written one proposal that I hope you will check out. My post is titled: “The Classification and Statistical Manual of Mental Health Concerns: An Alternative to the DSM that is Practical and Consistent with the Principles of Science.” http://dxsummit.org/archives/591
Keep up the fine work,
Jeffrey Rubin
LikeLike
Hi There, and welcome. and thankyou.
We had the idea floated at Now we’re all crazy- what next ” on Monday’s Mad Pride that since DSM is so obviously American, and since the way that we describe how we go mad has such a large cultural component, then maybe, being distinct from US, Canada needs to assert that difference and develop its own system….
A few folks are, even now and only semi non-seriously, plotting a trip to Boston to toss crate-loads of DSMs into the harbor as a symbolic act of independence from tyranny and of self determination….
I will certainly take a look at DX Summit and your ideas…
I’d say, as a general point, that the most important idea in any any classification system, and the first question to be answered, must be .
…what is it’s purpose?
k
LikeLike
I must say it was i interesting to read your post. You have some points, and I recognize the tendency to be sure that something must be wrong with how the patient takes the drug if they don’t get better. When it comes to psychological treatment, I really hope that there are some real benefits, and if the therapists ‘are as mad as the ones they treat, but living their life better’ that it at least can be a good thing, it really feels nice to have somebody who understands and cheers you on (isn’t that the whole role of a parent, giving children confidence while also teaching them about the world?) And if it is true, that the world makes us mad, wouldn’t it be better to give people motivation to do something about it? I think that when people are ‘healthy’ they want to make the world a better place, and much suffering in the world could have been done something with, if most people knew exactly what they should do. I highly recommend the movie/documentary about fear, which takes this theme to a interesting level : are the ‘leaders’ out there really doing what’s good for mankind? Like the drug companies who only care for profit. And if not, what can we do? It’s so wrong that there is so much suffering in the world, while some people are rich and not doing anything to make it better. Cheers to you, for asking a lot of important question, and for making it so understandable and easy to read. I think critical reflections like this, actually might be something that helps people, maybe we get less zombies because somebody read this 🙂
LikeLike
Hi Mirrorgirl and Welcome
Thanks, glad you liked my little rant.
maybe all we need if for more people to be full awake?
and to say “I’m not ok with this..”
It’s easy to tell ourselves the story that we can do nothing much – but doing what we can in our own lives is how, together, we change the world….
…and not that I’m against zombies but if reading this even one or two folks came to realise that living life as a zombie is not their only option then I would be very okay with that…
k
LikeLike
Love your thinking and cannot agree more! Cheers from someone who actually is naive enough to think that the world can be changed if we just come ‘together’ 😉
LikeLike
I fully agree! I keep a blog and have been saying all of the above in your article for the last 4 years. Believe it or not “autism” is also a made up illness and in my work with families and autistic adults, I have plenty of proof that it is being used just and only to spread terror and sell (more and more) drugs. The question is who is mad? The APA who comes up with make-believe mental disorders, or we the common people who think that these disorders are real?
That is a question that in the next few years more and more people will begin considering…
http://aspergermindspeaks.blogspot.nl/ (in English)
http://aspergerhellas.blogspot.nl/2013/05/dsm.html (in Greek)
LikeLike
That was wonderful..
LikeLike
Hi Christine
Thank you. Glad you like it.
K
LikeLike
Hilarious, and bang on! Best yet!
LikeLike
I LOVE your analogy of the Tylenol deficiency! It is a sad commentary on how drugged up society is. And we wonder why our kids reach for drugs instead of dealing with the problems instead?
LikeLike
Hi Denise
Thanks. I’m not sure if it’s entirely “mine”.
Dave Umbongo put a twist on it for sure.
I wonder how much our kids learned that from our example.
I remember vividly the day I heard my daughter [she was about six] ask her mom “how come Daddy takes so many pills?”
That was a big part of my waking up – realising how
much I’d swallowed that idea of being sick and needing medicine to manage it.
k
LikeLike