Love “One flew Over The Cuckoo’s Nest” ?
Want to see the remarkable story of how this remarkable movie was made?
Completely Cuckoo [documentary] tells that story.
A Mad For Movies
and Guattari Goes to the Movies Series Screening…
Completely Cuckoo
Watch the movie [87mins] then join in with a bit of a dialogue after.
Free
Tue 8th October
7pm to 9pm
U of T: Victoria College Building (Old Vic)
Room VC 323
73 Queen’s Park Crescent
Toronto, ON M5S 1K7
Accessibility: Venue is wheelchair accessible [- more info to follow here]
This event is brought to you by Community Partnership between:
UofT Comparatve For Literature
Guattari Research Group – Toronto
Recovery Network Toronto
ISPS-US.org [Toronto Branch]
About This Event
In partnership with Recovery Network: Toronto, ISPS-US, and the Centre for Comparative Literature, the Guattari Research Group – Toronto is screening Completely Cuckoo, the making-of documentary of One Flew Over the Cuckoo’s Nest, on Tuesday, October 8th, at 7:00pm in VC 323. The GRG – T is dedicated to investigating the work of Félix Guattari and its many different applications, interpretations, and mutations in various contexts within and beyond academia.
This is our inaugural “Guattari Goes to the Movies” crossover event with “Mad for Movies”. We’ve organized this screening in solidarity with Toronto communities in hopes of cultivating an open conversation about how we see our and others’ experiences and mental wellness. For more info about our community partner, Recovery Network : Toronto, and a short review about the documentary, please click the following link: https://recoverynet.ca/2019/09/25/completely-cuckoo-7pm-tue-8th-oct-2019/. We will have a short introduction and then a discussion after the film. All are invited and we hope to see you there!
“It was hard to discern who were the actors and who were the inmates,” says Christopher Lloyd of his time spent filming 1975’s Academy award-winning One Flew Over The Cuckoo’s Nest. It’s hardly surprising. As revealed in Charles Kiselyak’s excellent and often very funny feature-length documentary, we learn that the filmmakers and 89 mental patients effectively lived and worked together as one while shooting in a real-life psychiatric hospital in Oregon.
Viewers may detect a trend here: Merry Prankster Ken Kesey’s source novel had been written on the night shift in the ward of a Californian mental institution, while the author was high on Peyote, as a diatribe against what he coined “Bull**** consciousness” – the patients’ mental state, he believed, was a natural reaction to the soul-sapping insanity of corporate America and “institutionalised evil”. As Kesey, who clearly identified with his Goliath-baiting protagonist RP McMurphy, says, “Not only was I writing about these guys with twisted consciousness – but I had joined their ranks.” Years later, following a Kirk Douglas-starring stage adaptation and numerous knock-backs from queasy Hollywood execs, director Milos Forman would apply the same Dunkirk spirit to his movie, aided no end by a remarkably progressive administrator, Dr Dean Brooks, whose residential psychiatric hospital provided a location for cast and crew, and who insists the film-making process was a useful aid to his patients’ rehabilitation.
And it’s here that the real meat – and real heroes – of Kiselyak’s film begin to emerge. If leading man Jack Nicholson (absent here) described McMurphy as “a cross between Hamlet and Jesus Christ” in his Oscar acceptance speech, the people behind the cameras, including producer Michael Douglas and screenwriter Bo Goldman, reveal themselves to be no less unusual. All of which makes for a warm, and most moving hour-and-a-half.
I was lookin for affection
So I decided to go, swing that dick in my direction
I’ll be out of control
Let’s take it to perfection
Just you and me
Let’s see if you can bring the bring the bring the nasty out of me
Nownownow now sock it
Ooh ahh, sock it to me like you want to
I can take it like a pro and you’ll know
Do it long bro with a back stroke
My hormones are jumpin like a disco
I be poppin mats like some Crisco.
And all you gotta say is that Missy go
And when you say it though I want it moved slow
I’m at your house around midnight
Don’t fall asleep
It’ll just be me me me on a late night creep
I’ma show you thangs, that you can’t believe
Jump in this b-e-beat
And won’t you sock it to me?
Otherwise, if you want more info read on.
And come back here when you’re ready, pres that Big Purple Button.
How Good Is It?
Well, Here’s What Other Participants Had To Say About This Workshop..
“Wow! Just Wow!”
“Super-fabulous! Indispensable! Exciting!”
“Motivating! Skill & confidence-building!”
“The space created for the workshop was “safe enough” for me to take some risks and participate in ways that I might have otherwise not, had I not felt safe and supported in my learning environment.”
“I wanted a deeper understand of the role voices can play in trauma – I AM WELL ON MY WAY.”
“I resonate with mapping. This was a wonderful visual teaching tool for me personally in terms of contextualizing the “parts”.”
“Introduction to the framework was absolutely refreshing and exciting to learn about.”
“I am so grateful for this resource as a teaching tool.”
“Incredibly informative practical experience having the opportunity to interview Dave, The DrKens, and Woolfie. Many thanks for their willingness and participation.”
“This was a very liberating key idea: taking the position of curious observer, getting to know the voices as individuals in their own right with and individual narrative, story to tell, and knowledge to impart.”
“Knowing that there is an alternative framework, than typical medical model, which empowers both individual and worker to understanding and work with voice hearing.”
“It is an empowering, hope-instilling and successful framework. It doesn’t get better than that.”
“I learned it’s not about having tools or what we do, it’s about how we listen.”
Is This Workshop For You?
Do you…?
Work with people who hear voices and who struggle with their experience of that?
Have someone in your life who lives with difficult voices and who struggles with difficult experiences like that get called “psychosis?
Feel confident in your belief that voices are real and in your ability to offer acceptance and hope, to [de -ab]normalize difficult experiences andperson’s ability to make sense of their own experiences?
Feel weary of the notion that we must fear ourselves and fear each other?
Feel ready to take your next steps in supporting individuals in working with their voices ?
Feel ready to learn more, ask yourself “what else can I do?”.
Want to know more about how you can be part of creating a future worth living in, to join us in enacting a world that understands?
Are you ready to take your next steps?
If so, then this workshop might help you further tilt your universe and emancipate yourself with deeper understanding.
This workshop is designed to share useful material but mostly to help you be more open, curious and willing to learn about a person’s own experience – to deepen and broaden your own ability to understand so that you can join us in enacting a world that understands voice hearing, supports the needs of individuals who hear voices and views them as full citizens.
If more of us were able to work with voices then maybe fewer of us would need a career as patients.
Who this workshop is designed for…
Essentially this workshop is designed for workers who spend regular time with individuals who hear voices and struggle with their experience, including doctors, therapists, counsellors, peer-workers community workers
– anyone working in the health system, mental health services, social services, or with “the public”.
It can also be suitable for anyone who spends time supporting someone who struggles with voices and yet does not get paid for their work – and who wants to deepen and expand their own understanding of the roles voices can play in a person’s life, ways of understanding, key information, and ways of engaging that can support a person working with their voices.
So, if in your life you encounter people who struggle with the voices they hear and feel you need to understand, and you are ready to play your role in enacting a world that understands, then you may decide this workshop is for you.
Working with voices is always a choice that can only be made by the person hearing voices.
We open ourselves to exploring our own experiences using that to connect with others, willing to share our own vulnerabilities, yet always remembering and recognizing that it is the person we support who is doing the hard work.
This workshop will enable you better to…
Increase and deepen your own understanding of hearing voices as a normal human experience, maybe not shared by everyone, but part of what it means to be human.
Share information about who hears voices helping to demystify the phenomena and start conversations about how it is part of being human.
Develop a deeper understanding of the role voices can play in trauma/ woundedness.
Begin to work with approaches that can help discover how voices may be related to life struggles, offer powerful insight and clues to what a person can do to make changes.
Offer yourself as guide or partner for a person you support – walking alongside a person who chooses to work with the voices they hear.
Work with practical approaches for working with voices that can enable a person to find their power to reclaim their life and make changes in their own experience.
Reflect on and share your own challenges, learning, assumptions, and growth as a human being and in any of your roles.
If, after participating in Accepting Voices Workshop you have been offering yourself as a “one-person-safe-space” and you find yourself privileged by someone taking you up on your offer and asking you to walk alongside them as they do their work, then you might find yourself asking …
“ok what’s next?”
“what kind of things might we do together?”.
This workshop is about just that, offers you an introduction and enables you better to:
Share your unshakeable belief that voices can be understood in simple terms and in context of life- a whole life.
Support people who have chosen to do the sometimes difficult work of emancipating themselves, and learning to make changes in their relationship with difficult experiences that they live with.
Share ideas and support a person by sharing selecting and working through practical approaches that enable them to explore, name, and make sense of their uniquely personal experience, to reclaim and use their power, and to write a new story of their life.
Includes introduction to and practical hands on experience using :
Voice Mapping
Voice Profiling
Maastricht Interview
Voice Dialogue,
Non-Violent Communication.
Workshop design…
This is an intensive, highly practical and experiential workshop- a learning circle in which we learn with and from each other and reflect deeply on our experiuence.
We will share a number of approaches that can be used singly or in any combination but the real learning comes from how we engage together. For each of the approaches we will…
S hare key ideas, tools and resources;
Immerse ourselves in practical exercises to explore
The approaches and techniques
Engage in deep personal reflection, shared sense making and dialogue…
A Creative Approach
This is not presented as therapy or a manualized approach but the material and ideas do lend themselves to being integrated into counselling or therapy work; some are structured, some very intuitive, iterative and creative.
This work is not so much with adhering to techniques, or following steps as seeing these approaches as ways to build relationship, explore, learn together, always letting the person you support take the lead, make choices, find and use their power.
A Framework / A Map
The Map For Reclaiming Our Power introduced in Acceptingf Vocies and based on work by Dr Marius Romme, is a key tool for navigating the landscape as we walk alongside a person who choses to work with their voices
Topics Included
Holding Safe-enough space
Voices and Trauma
Voice Mapping
Voice profiling
Maastricht Interview
Non-Violent Communication
Voice Dialogue
Presenters
Kevin Healey
Has been hearing voices for over forty years and for almost ten has played a key role in establishing Hearing Voices Network in Toronto and supporting others do the same where they live in Canada.
Founder and facilitator for the Toronto Hearing Voices group, one of the longest running in N. America.
Collaborating with artist Dora Garcia founded Hearing Voices Café, Toronto – the world’s first as a regular feature in a city landscape, followed by others now in Valladolid and [coming soon], Paris and London.
Dave Umbongo
For years Dave would only say only one word, now he authors articles at http://www.recoverynet.ca and talks non stop..
Voices have stories too.
Dave doesn’t really have a bio – like other superheroes he has an “Origins Story”,
and like “THE TRUTH” some of it, at least …
“ . . . . . .IS OUT THERE.”
Too often, we regard listening as waiting for an opportunity to interrupt.
Or else as ‘active listening’: that weirdly fidgety preoccupation of mentally checking off a checklist list of ‘shoulds’ and ‘should nots’, endless micro-tyrannies we can obey and designed to make us believe we look like we’re listening.
And, yet listening can itself be healing.
Q. What does it mean to really, really listen?
Q. How does it feel when we do?
Q. How does it feel to be really listened to?
We will share simple ideas that we can use to begin listening more fully.
We will practice grappling with each and we will reflect together on our expériences.
That’s it.
And it will be enough: because listening – really listening – is healing,
and healing is hard work.
Thursday 27 Feb 2020 930am to 1pm
Facilitator:
Kevin Healey
Location:
Boardroom, 4th Floor
Inner City FHT
69 Queen St E
Toronto
These are difficult times and this is difficult work: how might we approach it first as human beings?
Escalation is a dynamic that involves at least two people.
We all “escalate“: in response to [something in] our environment, and in context of our whole life experience.
Whatever a person is doing is both an expression of a deeply felt need, and a survival response.
Whatever survival response we tend to fall back on is likely one that we’ve learned from how life has treated us and one that’s worked so far… but is also not the only one and may not the best one for this moment.
The only person I can “de-escalate” is me.
How do we draw upon experiences of being in the role of worker required to “de-escalate” a person said to be “in need of de-escalation”?
How do we draw upon experiences of having been that person said to be “in need of de-escalation”?
How might we go beyond the operationalisation, steps and rules-based approach of “de-escalation” and instead UN_ESCALATE?
A concentrated half-day WORKshop for WORKers…
Sharing ideas and practical stuff you can use to suck less.
Limited Spaces. Small Groups
Thu 20 Jan, 2020
9:30am to 1.00pm
Fee $75
Facilitator:
Kevin Healey
Location:
4th Floor, Board Room
69 Queen St E, Toronto
Register online NOW
Registration is online at eventbrite.
Click on the link below or on the BIG PINK BUTTON
Article from Samantha McCabe at Globe & MAil on how City of Toronoo’s latest approach to offereing refuge from heat falls short.
Experienced RNs and Street Nurses Roxie Danielson, Cathy Crow, Joyce Rankin speak to how it impacts health and lives of those less fortunate and John Neapean offers a personal account of what its like being told by the City’s website to go to splashpools to cool-off, only to be threatened when he does with tresspass and arrest by city’s staff and police officers.
“Toronto the good” never sounded so hollow.
Dear Torontonians: This is on us – on all of us.
Toronto’s heat-relief network not enough to cool city’s most vulnerable, health and outreach workers say.
photo: CHRISTOPHER KATSAROV/THE GLOBE AND MAIL
SAMANTHA MCCABE
Globe and Mail,
Roxie Danielson, an RN who works as a street nurse, is greeted by a client that she hasn’t seen in six months in Toronto.
Sunlight beats down on the pavement of Toronto’s Yonge-Dundas Square. Throughout the square, people sit on the ground, framed by only thin slivers of shade.
As usual, they have coffee cups beside them to collect change, but today, many are asking passersby for something else: a bottle of water.
Homeless people, more than anyone else, are vulnerable to the elements – a concern the city of Toronto is familiar with, as every winter those left out of crowded shelters face plunging nighttime temperatures. But street nurses, outreach workers and others say that the city’s strategy to address the issue, while evolving, is undermined by a misunderstanding of what it’s like to be homeless in summer weather.
This year, Toronto’s City Council and Board of Health decided to close seven “cooling centres,” air-conditioned buildings that were open on days the city issued hot-weather warnings, which occurs when two or more consecutive days reach temperatures of 31 C or warmer. One location was open 24 hours a day. The centres had been operational since 2002, employing some staff who were formerly homeless, and offering water, snacks and transit tokens for people to get to the centres and back.
Instead, they have continued on with a pilot project launched last summer: a “heat relief network,” which is a system of existing public spaces anyone can find via an online map, which the city says is based on models used in other large urban centres such as New York and Arizona.
The heat-relief network does not create new, dedicated support locations, but rather increases the visibility of existing resources.
“I have no problem with the city advertising more cooling spaces,” said Cathy Crowe, a long-time street nurse, activist and educator. But she called the closing of the centres “beyond frustrating” and said many of the network’s 300-plus locations – such as malls, community centres, splash pads and public pools – are problematic for housing-vulnerable populations.
Joyce Rankin, the clinical manager of homeless outreach organization Street Health’s Dundas location, has been working with downtown Toronto’s most vulnerable people for a decade. She dubs heat the “silent killer” on the streets.
Fourteen-hour days spent exposed to scorching heat presents a long list of hazards, of which dehydration is just the beginning. Extended exposure to hot weather exacerbates existing cardiac and respiratory problems. It can also be a dangerous complicating factor for those with substance-abuse issues or on medications.
And it’s getting worse as climate change contributes to more extreme weather patterns and urban heat climbs.
John Nepean, who recently secured a spot with Toronto Community Housing but was homeless for years before that, was recently walking around the city on a sweltering day. He spotted a splash pad – the likes of which are advertised on the heat relief network – and took his socks and shoes off to wade in.
A woman nearby called the police.
“They told me I either leave or I could be arrested for trespassing,” Mr. Nepean said.
There’s an urgent need to provide better care, says Roxanne Danielson, who works with homeless and formerly homeless people as a member of the Inner City Family Health Team.
“We can’t have just pools and splash pads where people are just getting kicked off by police. We need designated spaces for people.”
The city’s goal is to better serve people by maximizing the use of publicly available cool space. “The intent is to continue to expand the network to provide heat relief to residents and visitors all summer and not just during … heat alerts,” according to Gayle Bursey, director of healthy public policy for Toronto Public Health.
Mr. Nepean described the difficulties he faced during his long stint of homelessness. He said that the cooling centres used to be the friendly, open-door place to go.
“You’re not judged on what type of person you are …” he said of the cooling centres. “That makes a difference.”According to Ms. Bursey, the cooling centres were “not well-used by the intended population.” She did not elaborate about the level of use.
A 2018 memo from the city’s Medical Officer of Health notes that during Toronto’s “uncharacteristically cool summer” in 2017, the cooling centres were only open on seven occasions, but still saw 2,714 visits across those days.
At a workshop hosted by Toronto Public Health that same summer, advocates for the facilities agreed underuse was an issue, but stressed the importance of maintaining centres where people could access food and health care and would not be pressured to leave. They further argued the city should work to make people aware of this resource.
After what they saw as a productive listening session, the move to axe the cooling centres two years later comes as a surprise.
This year, Toronto has increased its budget for hot weather response, to $118,000 from $85,000 last year. More than half of that budget – $65,000 – was transferred to the Shelter, Support and Housing Administration to pay for additional staff who have experienced homelessness: On heat-warning days, Fred Victor Centre has been contracted to send teams of two to each of Toronto’s four 24-hour respite sites to patrol the nearby streets and supply people with information and water. Respite sites offer overflow spots as a response to full shelters.
This summer, there are 429 spots across respite sites, down from 515 last summer and way down from this past February, when the city provided 805 respite site spots after a hard push for more accommodations during harsh winter temperatures.
Those 429 spots are regularly at almost full capacity alongside an overburdened shelter system.
NO ROOM AT THE SHELTERS
There is so little room at Toronto shelters and overflow sites that during the six hottest days of the summer,capacity was at more than 98%.
At shelters, the city has added 351 beds since February as part of its spring transition plan, but when the lost respite spots are accounted for, the overall number of beds has dropped by 125.
“Generally, people know what services are out there,” said Greg Cook, an outreach worker with Christian charitable organization Sanctuary. “The issue is there’s not more services by and large, [and] that ever ything is full. … So what are you actually connecting people to?”
There is no long-term solution to getting people out of these outdoor conditions, Mr. Cook said, making outreach difficult.
At the end of the summer, Toronto Public Health says they will review the successes and challenges of the heat relief network. They will then report to the Board of Health and propose a “long-term strategy for the city,” according to a spokesperson.
Advocates say the root of the issue is obvious: The lack of affordable housing in one of Canada’s most expensive cities.
“The really important piece is to understand that we’re in a climate crisis, and this is only going to get worse,” Ms. Danielson said.
Opinion piece by Richard A Friedman in NYT, 8 Aug 2019.
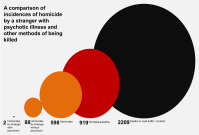
The current [and for some while] habit of dismissing mass murders as acts of “mentally ill monsters” has no basis in anything but unthinkin predjudice and habitual hatred – ironically of the same kind that drives many of these acts.
Richard A. Friedman shows how those who act in such ways are like any of us, and can become consumed by hatred.
“Perhaps there is a beast
…maybe it is us.”
– William Golding
Large scale studies have shown that only a minority of “mass murders” [typically classified by researchers as homicides of 4 or more people] are conducted by people who diagnosable wiuth “mantal illnbess”.
As Friedman says it …
people in the grip of ordinary emotion are capable of carrying out heinous acts of violence; you don’t need to have a mental illness to be a “monster.”
And
The scary truth is that ordinary human hatred and aggression are far more dangerous than any psychiatric illness.
And when it comes to blind faith in mental health services and the belief system at their core- psychiatric diagnosis – has as magical powers to predict acts of violence…
The notion that we can identify mass killers before they act is, as yet, an epidemiologic fiction.
Experienced psychiatrists fare no better than a roll of the dice at predicting violence.
The monster is [within] us.
How true it is that we need more psychiatrists and others “mental health professionals” to be so honest.
Why Mass Murderers May Not Be Very Different From You or Me
Most of them are not mentally ill. They are just filled with hate — and well armed.
CreditIllustration by Nicholas Konrad; Photographs by The Image Bank/Getty Images and Rob Curran, via Unsplash
After a gunman massacred 22 people in an El Paso Walmart last week, President Trump declared that mass killers are “mentally ill monsters.”
It was a convenient — and misleading — explanation that diverted public attention from a darker possibility behind such unimaginable horror: The killer might have been rational, just filled with hate.
It’s reasonable to think that anyone who guns down 22 human beings in cold blood must be deranged or de facto have a mental illness. But the truth about mass killers and the link to mental health is more complicated than that.
One of the largest studies of mass killers, conducted by Dr. Michael Stone and involving 350 people, found that only 20 percent had a psychotic illness; the other 80 percent had no diagnosable mental illness — just the everyday stress, anger, jealousy and unhappiness the rest of us have.
Sign up for David Leonhardt’s newsletter
David Leonhardt helps you make sense of the news — and offers reading suggestions from around the web — with commentary every weekday morning.
Likewise, an F.B.I. study of active shooters between 2000 and 2013 found that only 25 percent had ever received a psychiatric diagnosis and just 5 percent had a psychotic illness.
(Some of my psychiatric colleagues like to point out that mass killers commonly have histories of being physically and sexually abused. Sure, but given the prevalence of such abuse in America, it seems obvious that a vast majority of traumatized people do not turn into mass killers.)
Still, the clear implication of these findings is that people in the grip of ordinary emotion are capable of carrying out heinous acts of violence; you don’t need to have a mental illness to be a “monster.”
We can’t know for sure whether the suspect in the El Paso killings, Patrick Crusius, 21, was mentally ill without detailed knowledge of his personal and medical history. But his online writing suggests we should not be so fast to assume that he is.
In a manifesto attributed to him, Mr. Crusius railed against immigration, described a plan to separate America into racially distinct areas and warned that white people were being replaced by foreigners. He said that “this attack is a response to the Hispanic invasion of Texas.”
To me, the statement appeared logical, coherent and not particularly rambling or delusional. Strikingly, the manifesto seemed to echo what Mr. Trump has been saying all along about immigrants. For example, at a recent Florida rally the president said, “You look at what is marching up, that is an invasion!”
Seen from this perspective, it is entirely plausible that the El Paso killer is a rational person who happens to be inspired by a hateful racist ideology.
The scary truth is that ordinary human hatred and aggression are far more dangerous than any psychiatric illness. Just think of the many people driven to mass murder because they were fired by employers or dumped by girlfriends. In all likelihood, they were not mentally ill but simply full of rage — and well armed.
In fact, mental illness contributes to about 3 percent of violent crime in America. The best evidence shows that there is a very small increase in the risk of violence only for those with serious mental disorders like bipolar disorder and schizophrenia.
The notion that we can identify mass killers before they act is, as yet, an epidemiologic fiction. These individuals typically avoid contact with the mental health care system. Even if they didn’t, experienced psychiatrists fare no better than a roll of the dice at predicting violence.
Other mass killers bear this out. Brendon Tarrant, who murdered 51 people last March in a mosque in Christchurch, New Zealand, was found at trial not to be mentally ill. Rather, he was a white supremacist who planned his carnage for two years and was driven by an anti-immigrant and racist ideology similar to Mr. Crusius’s. And like Mr. Crusius, he believed in a white supremacist conspiracy theory called “the great replacement,” which posits that white Europeans, with the complicity of “elites,” are being replaced by non-European people through mass immigration.
Then there is Dylann Roof, who murdered nine people in 2015 in a church in Charleston, S.C. He too espoused racial hatred in an online manifesto. Though he was given a diagnosis of social anxiety disorder and mild autism by an evaluating psychiatrist, neither of these diagnoses involved a state of psychosis that might have rendered him unable to comprehend the nature of his actions.
Judging from their manifestoes, you have to wonder whether, at the very least, these killers expected social approval from those who shared their racist ideology, to say nothing of a desire for fame.
Given the global resurgence of white nationalism and xenophobia in recent years, is it really surprising that a few individuals have responded to this climate of hate by violently channeling such ideas? After all, we are social animals who are easily swayed by our environment. And that environment is awash in rage these days.
What this suggests is that bolstering mental health programs — while a worthy goal — will not solve our mass shootings epidemic. More effective policies might involve gun control, including enhancing background checks and expanding so-called extreme risk protection orders, which would allow law enforcement to temporarily remove firearms from people deemed potentially violent.
This should scare the hell out of all of us. The next mass killer is out there — somewhere — watching very carefully what we say and do to one another. And he may be as sane as you or me.
Richard A. Friedman is a professor of clinical psychiatry and the director of the psychopharmacology clinic at the Weill Cornell Medical College, and a contributing opinion writer.
Trauma is not what happened in the past but it is about how we experience what happens now.
How we experience this moment is shaped by how we experienced every moment we experienced before this one.
If we experience event that threaten our safety in a state of helplennsess we can becom etraumatised- wounded. to b etraumatised – wounded- means we live our live fro mthis moment in a different body, different mind, different relationship with the world.
The ways in which this can affect us and our health are unlimited and challenge medical understanding and mdical diagnostic categorisation.
Resilience grows from adversity too, we will move through life with our own trauma burden and resilience reportoir, some combination of both that is unique to us, shaped by our unique experience of the world.
Trauma is not what happened, it is the wounds we carry from how we experience being in the world..
These wounds shape how and who we are in this moment. Wounds can heal, how do we learn to heal?
How do we learn to supoport each other in our healing?
“In western medicine we mistakenly categorise trauma by what happened
when in fact it is the effect left within us from our experience.”
Robert Scaer
In this conversation Robert Scaer talks about how he came to his understanding of how trauma works in the mind brain body continuum covered in his books.
The Body Bears The Burden
Trauma, dissociation and disease.
Originally written for Doctors. In hope that some reading it might change their minds.
In the vid you’ll hear him talking about 1st edition -writen for medical professionals, 2nd edition revised for ordinary folks [non doctors]. There is also now a 3rd Edition.
The Trauma Spectrum Hidden Wounds and Human Resiliency
– which as you’ll here he originally wanted to call:
“Trauma Tells The Tale: Understanding your life”
“because I felt by this time that trauma was ubiquitous. It was in effect, in all of us in some ways, that every body experiences phenomena in their lives and that it had a profound effect on all of their life’s choices.”
The New Traumatology and The trauma Spectrum | Part 1
The New Traumatology and The trauma Spectrum | Part 2
When even The Telegraph calls it domestic terrorism then …
Imagine living in a country where even going to the mall means you could get shot for the colour of your skin, religion, gender or…
Then when you struggle and seek help you get told its because there is something wrong with you.
Surely, the very definition of living in a terrorist state, and services that do this are complicit in creating such a state.
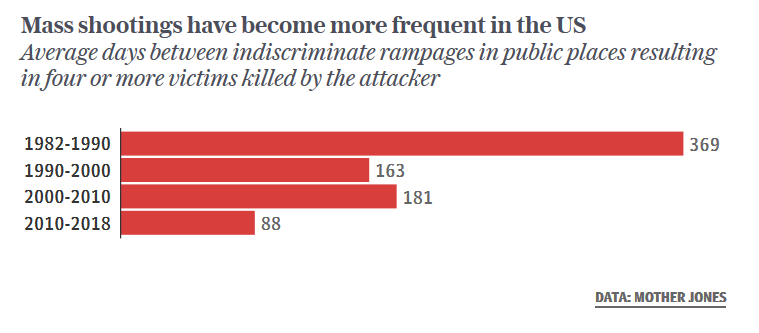
The chart from, The Telegraph, shows how the average number of days between random mass shootings in US has been dropping, including a dramatic drop in the latest decade.
Article describing how us laws framed to enable FBI to surveill and track actors connected with foreign powers make it very difficult to track internal actors inspired by a incumbent to the office of president who openly spouts his white supremacist ideology.
And how a intelligence services in focussing on foreign threat totally took their ey eof fteh ball on internal threat even as it grews and became the greater threat…

 Love “One flew Over The Cuckoo’s Nest” ?
Love “One flew Over The Cuckoo’s Nest” ?









 The Trauma Spectrum
The Trauma Spectrum